Reversible Unilateral Tongue Border Atrophy Associated With Anti-Acetylcholine Receptor Antibody-Positive Myasthenia Gravis
Dec-25
Abstract
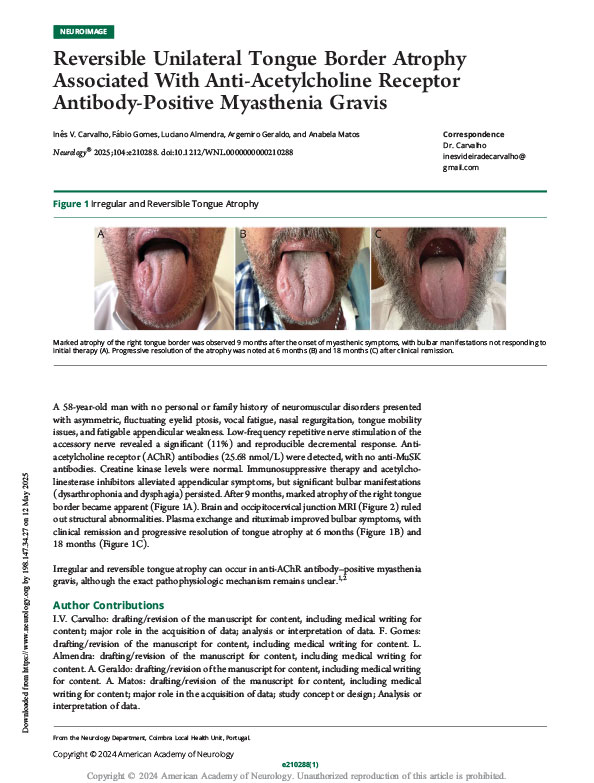
A 58-year-old man with no personal or family history of neuromuscular disorders presented with asymmetric, fluctuating eyelid ptosis, vocal fatigue, nasal regurgitation, tongue mobility issues, and fatigable appendicular weakness. Low-frequency repetitive nerve stimulation of the accessory nerve revealed a significant (11%) and reproducible decremental response. Anti-acetylcholine receptor (AChR) antibodies (25.68 nmol/L) were detected, with no anti-MuSK antibodies. Creatine kinase levels were normal. Immunosuppressive therapy and acetylcholinesterase inhibitors alleviated appendicular symptoms, but significant bulbar manifestations (dysarthrophonia and dysphagia) persisted. After 9 months, marked atrophy of the right tongue border became apparent (Figure 1A). Brain and occipitocervical junction MRI (Figure 2) ruled out structural abnormalities. Plasma exchange and rituximab improved bulbar symptoms, with clinical remission and progressive resolution of tongue atrophy at 6 months and 18 months.
© 2026 Wolters Kluwer. All right reserved.